The most common surgical abdominal incisions are explored here.
When making a surgical incision, the surgeon must attend the following key principles whenever possible:
1. Try to follow Langer’s lines for maximal wound strength with minimal scarring;
2. Try to split the muscles instead of cutting them.
Laparoscopic procedures are increasingly the common option for abdominal surgeries, as they generally present better results in terms of aesthetics, postoperative pain, recovery time and length of stay. However traditional open approach are still required in some situations and the most common incisions are explored here.
The most common Abdominal Incisions:
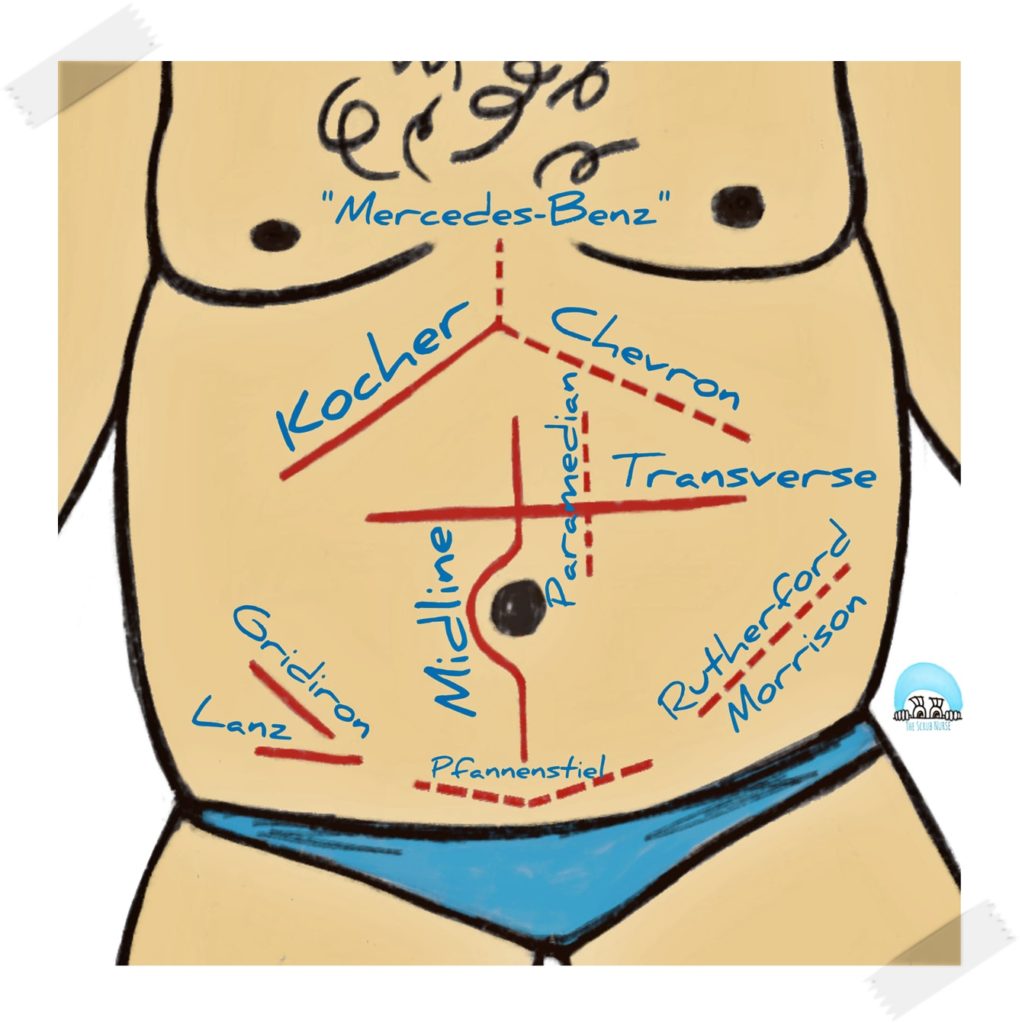
- Midline incision: incision that follows the linea alba (a relatively avascular structure) to access most of the abdominal viscera; performed on a wide variety of abdominal surgeries, including emergency procedures, as this incision causes minimal blood loss; the downside is the susceptibility of significant scars.
- Paramedian incision: incision 2-5cm lateral to the midline; used to access mostly the lateral viscera (such as kidneys, spleen, and adrenal glands); the anterior rectus sheath is separated and moved laterally, preventing any division of the rectus muscle; however this approach takes a long time and is often technically difficult; it also can damage blood and nerve supply of the muscles, which may result in the atrophy of the muscle; this technique is rarely perform in the UK.
- Kocher incision: subcostal incision made parallel to the costal margin, starting below the xiphoid and extending laterally; used to access the gall bladder; these subcoastal incisions provide good abdominal viscera exposure and good healing. Other variations of Kocher incision are:
- Chevron / rooftop incision: the extension of the incision to the other side of the abdomen; used to access the oesophagus, the stomach, and the liver.
- Mercedes Benz incision: Chevron incision with a vertical incision and break through the xiphisternum; same indication as Chevron incision, but mostly performed in liver transplantation.
- Transverse Incision: they vary in size and location; when a full-length transverse incision is made some muscles (the oblique, the transverse and the rectus abdominis) and linea alba are cut in a horizontal plane, causing more blood loss than the midline incision and being more time-consuming; surgeons may also perform smaller transverse incisions and remain unilateral.
- Supraumbilical transverse incision: offers excellent exposure of the upper abdomen;
- Pfannenstiel incision: infraumbilical transverse incision in the lower abdomen; mostly used for gynaecological and obstetric procedures. The skin is incised transversely, often with a convexity downward to avoid dissection of blood vessels and nerves.
- Lanz incision and Gridiron incisions: used to access the appendix, mostly to perform appendicetomy; both are made at McBurney’s point. In comparison to Gridiron incision, Lanz incision produces better aesthetics results with reduced scarring as it follows the Langer’s lines.
- Rutherford-Morison incision: similar with the Gridiron incision but the surgeon extends the incision into an oblique and curvilinear orientation, facilitating access to the ascending colon and sigmoid; also used for kidney transplantation.
References:
Geeky Medics – Abdominal Surgical Incisions
TeachMeSurgery – Abdominal Incisions in General Surgery
Scandinavian Journal of Surgery – Abdominal Incisions: Techniques and Postoperative Complications
Surgery (Oxford) – Abdominal access techniques (including laparoscopic access)